News about the malformation of the C6 and C7 vertebrae has understandably raised a lot of concern. There are major implications for both buyers and breeders of TB and TB-derived breed horses, as outlined in the original article, All You Need to Know About the Hidden C6-C7 Malformation That’s Bringing Horses Down. In response, Sharon May-Davis has very kindly provided us with the English version of a paper she published in the Journal of Japanese Local Government Racing, outlining a preliminary protocol for radiographing this area of the neck and identifying the malformation. (Yes, a single racing authority has taken this issue on board!)
So without further ado, here is the paper in its entirety, the only adaptations being the positioning of images to better fit this site’s blog format.
© All text copyright of the published authors. No reproduction of partial or entire text without permission. Sharing the link back to this page is fine. Please contact me for more information. Thank you!
Preliminary Radiographic Protocols for Identifying Congenital Malformations of the Caudal Cervical Vertebrae
Authors: May-Davis S.E.R., Minowa F., Monoe S.
Abstract
In 2014, a published study based on dissections and skeletal examinations noted that 19:50 Thoroughbred horses had a congenital malformation of the 6th cervical vertebra (C6). In addition, it was found that in those 19 Thoroughbred horses expressing a congenital malformation of C6, 9 displayed a concurrent congenital alformation of the 7th cervical vertebra (C7). In this study, 3 Thoroughbred horses and 1 Thoroughbred type were clinically examined; 3 were radiographed for limb abnormalities and 2:3 radiographed for the congenital malformation of C6 and C7 prior to euthanasia. Upon dissection, 3:4 expressed a congenital malformation of C6 with 2:3 displaying a concurrent CM of C7. These 2 horses were positively radiographed for the CM of C6 and C7 prior to dissection. The radiographs of C6 were taken in direct lateral orientation with 0 degree of elevation and revealed the absence of the caudal ventral tubercle (CVT) of C6. Re-positioning the horse’s forelimbs caudally with an outstretched neck, C7 was radiographed at a 30° oblique lateral angle in a cranial to caudal direction with 0 degree of elevation; the transverse process of C5 remained cranial to the beam. The caudal aspect of the plate was positioned medial the Cranial deep pectoral and rotated vertically to expand the field of view of the cervical vertebrae, whilst remaining perpendicular to the beam.
Introduction
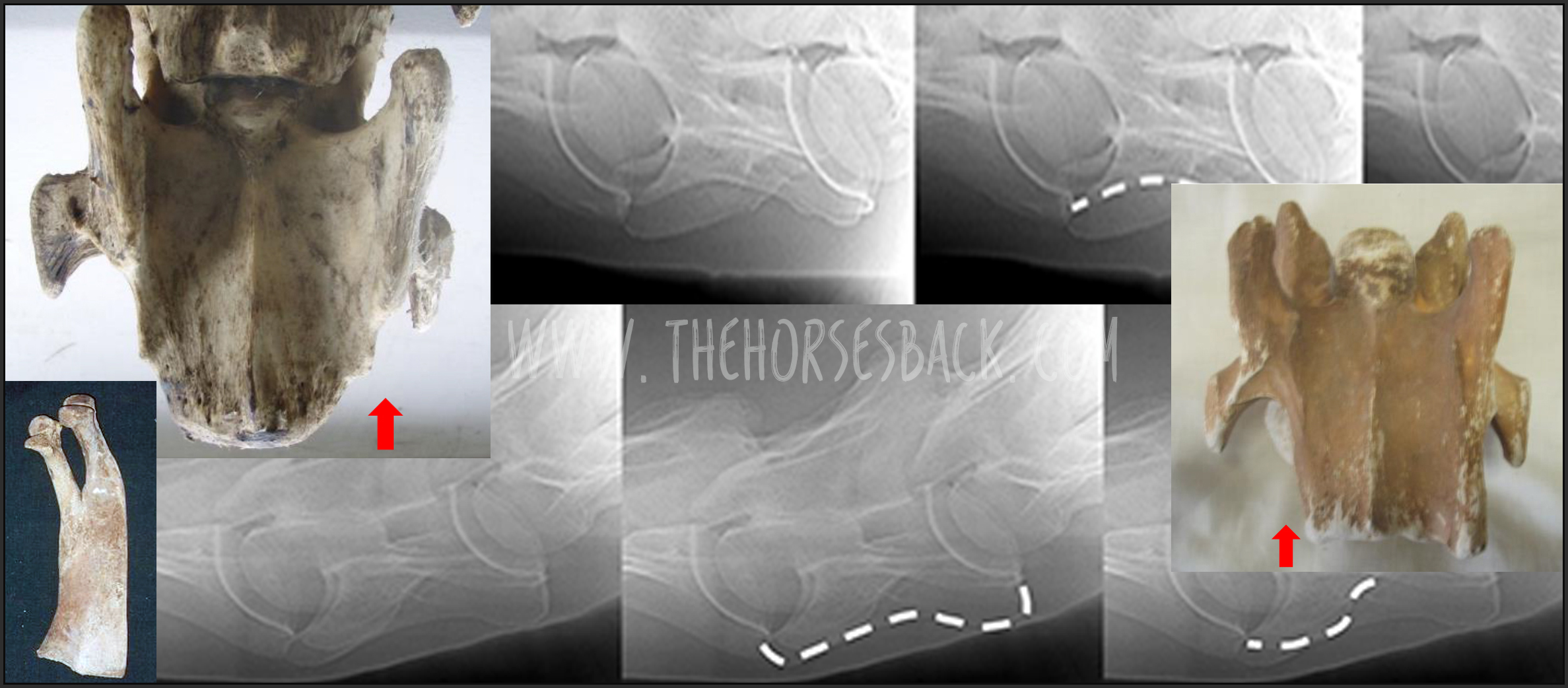
In recent times, 3 Australian studies reported congenital malformations of C6, C7, the 1st sternal rib, along with their associative soft tissue structures. Furthermore, it was noted that these congenital malformations were predominantly breed related and more specifically, to Thoroughbred horses or derivatives thereof. In addition, reports of forelimb proprioceptive dysfunction, neurological impediment and gait deficits were concurrently noted (May-Davis [a,b], May-Davis and Walker). The congenital malformations of C6 appeared as either a left or right unilateral absence of the caudal ventral tubercle (CVT) or as a bilateral absence of the CVT (Figure 1).

Figure 1. View of the ventral aspect of C6, cranial aspect top. Photo credit: Sharon May-Davis
The congenital malformation of C7 appeared with either a fully transposed CVT from C6 onto the ventral surface of C7 or a partial transposition of the CVT from C6 onto the ventral surface of C7 (Figure 2) (May-Davis [a]).

Figure 2. View of the ventral aspect of C7, cranial aspect top. Photo credit: Sharon May-Davis
The congenital malformation of the 1st sternal rib appeared in multiple presentations with gross anatomic variations including; an absent 1st sternal rib; bifid Tuberculum costae (Figure 3); bifid Sternochondral articulation onto the sternum; flared shaft; normal 1st sternal rib inserting onto the cranial branch of a bifid Sternochondral articulating 2nd sternal rib; straight costal shaft and an articulating rudimentary Tuberculum costae with a ligamentous extension replacing the bony shaft and attaching to a rudimentary Sternochondral articulation onto the sternum (May-Davis [b]).

Associative soft tissue structures varied according to the presentation of the congenital malformation with the most noted being, the Longus colli muscle, Scalene muscles and neural vessels such as the Phrenic nerve and Brachial plexus (May-Davis [b], May-Davis and Walker).
The congenital malformations noted in these 3 studies were determined via dissection and skeletal examination. They were based on 2 specific skeletal variations in C6 and C7 plus any variation to normal of the 1st sternal rib.
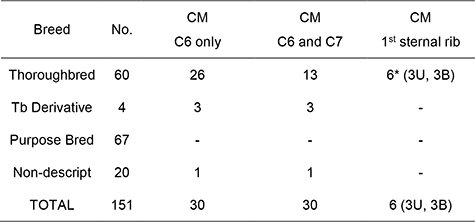
The congenital malformations could appear in C6 as a singular expression with no other anomalies, however, the congenital malformation of C7 only occurred when the CVT was absent on C6. The congenital malformations of the 1st sternal rib only occurred in the presence of the congenital malformation of C6 and C7 (Table 1) (May-Davis [b]).
With this in mind, the premise that if a congenital malformation exists in C6 then there is a 50% chance that transposition will occur on C7. In this format, it would stand to reason that there could also be an anomalous rib. Therefore, this study is designed to identify the absent CVT on C6 and investigate its transposition onto C7.
Materials and Methods
After evaluation and clinical examination, the 2 horses (1 Thoroughbred and 1 Thoroughbred type) were restrained in cross ties. Detomidine Hydrochloride (Detomovet CEVA Animal Health Pty Ltd) was administered via left jugular vein venepuncture. The dosage was determined by the clinician’s experience and in consideration of the individual’s current health status.
The radiographs were obtained by utilising a Porta 100 HF High Frequency portable x-ray unit (7.8kgs). The kV range was 40-100kV with an mA range of 20-30 mA and a mAs range of 0.3 – 20 mAs. The images were captured on a wireless Rayence 1012WCA Medical Image processing unit (26cm x 32.5cm) and computerised with Vetview Digital Diagnostic Imaging software.
The radiographic angles were obtained with the horse’s neck in full extension and the forelimbs behind the vertical in standing position. With the clinician standing with the x-ray unit on the left side of the neck and the plate positioned on the right side of the neck, the distance between the x-ray unit and plate was 80cms. The x-ray unit and plate remained lateral to the cervical vertebrae determined by the transverse processes of C5.
The first view is a direct lateral at 90 degrees, with 0 degree of elevation whilst maintaining the transverse process of C5 to the left of the beam.
Remaining lateral to the cervical vertebrae with a 0 degree of elevation, the second view is taken with the x-ray unit positioned at a 30° oblique lateral angle in a cranial to caudal direction with the transverse process of C5 cranial to the beam. The caudal aspect of the plate is positioned medial the Cranial deep pectoral and rotated vertically to expand the field of view of the cervical vertebrae, whilst remaining perpendicular to the beam.
Upon the radiographic evaluation of C6, radiographs of C7 are obtained. The 4 horses were then euthanized and dissected so to verify the radiographic findings. Only those pertaining to the congenital malformation of C6 and C7 are reported in this study.
Results

Upon euthanasia of the 4 horses, Thoroughbred No.1 was normal. Thoroughbred No.2 presented with an absent CVT in C6 and trachea compression (Figure 4).
Thoroughbred No. 3, presented with a C6 and C7 congenital malformation and a malformed 1st sternal rib. The Thoroughbred type also presented with a congenital malformation of C6 and C7 (Table 2).
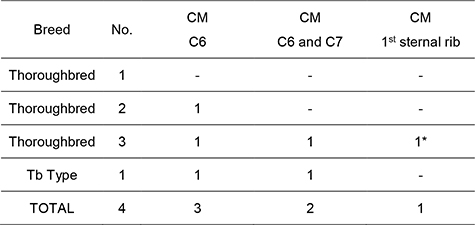
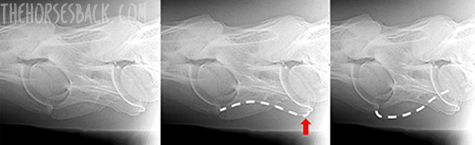
Figure 5. The radiographic lateral view of C6 depicting a unilaterally absent CVT in C6. Image credit: Sharon May-Davis
Thoroughbred No. 3 C7 radiograph (Figure 6) clearly presents the observer with a transposition of the CVT from C6 onto the ventral surface of C7, furthermore it denotes a reciprocal deviation in the trachea at the point of this transposition.
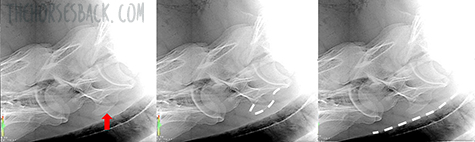
Figure 6. The radiographic view of C7 depicting a unilaterally transposition of the CVT from C6. Image credit: Sharon May-Davis
The Thoroughbred type (Figure 7) exhibits the absent CVT in C6. The radiograph clearly indicates an absent CVT that is unilateral in its presentation.

Figure 7. The radiographic lateral view of C6 depicting a unilaterally absent CVT in C6. Photo credit: Sharon May-Davis.
The Thoroughbred type C7 radiograph (Figure 8) clearly presents the observer with a transposition of the CVT from C6 onto the ventral surface of C7, furthermore it denotes a reciprocal deviation in the trachea at the point of this transposition.
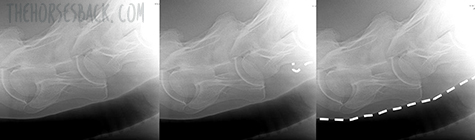
Figure 8. The radiographic view of C7 depicting a unilaterally transposition of the CVT from C6. Photo credit: Sharon May-Davis.
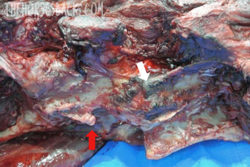
Upon dissection, the Thoroughbred type displayed identical congenital malformations of C6 and C7 as depicted in the radiographs (Figure 9).
Discussion
This study was conducted with the view to obtain specific radiographic evidence of the congenital malformation of C6 and C7. Radiographic views of the 1st sternal rib were not possible due to thick and dense musculature in the region. The views obtained of C6 and C7 with exact radiographic angles proved that this region can be radiographed with precision so that the practitioner can make a clear diagnosis should a horse present with a neurological deficit, as previously published (May-Davis
[a, b], May-Davis and Walker]). Furthermore, the asymmetry of the cervical vertebra could exacerbate arthritis in the articular process joints as previously noted (May-Davis [a]). In addition, the incidental finding of the compression of the trachea is an important factor to consider when Thoroughbred racehorses present with compromised airways. An explanation for this occurring is that the Longus colli muscle hypertrophies in support of the weakened structures and due to its proximity to the Trachea, it impinges upon its dorsal surface. This impingement is further exacerbated by the ventral projection from C7 of the transposed CVT from C6.
Since the first publication in 2014, retrospective studies were conducted that added another dimension to the current research. Italian and American studies noted that Warmbloods, Quarter Horses and Arabs were also afflicted with this condition (Santinelli et. al 2016 and DeRouen et.al 2016). It is significant to note that these breeds present the majority of the ridden horse population in Japan extending from Racing, Showjumping, Dressage to Eventing and Endurance. However, a specific Dutch Warmblood study was conducted with fresh cadaver’s that were portioned and CT scanned (Veraa et.al 2016), this also included Oldenburg horses. The congenital malformation of C6 and C7 was present in both breeds with a noted malformed 1st sternal rib in a Dutch Warmblood. Combined percentages of these 3 studies in conjunction with the 3 Australian studies and the current study has the congenital malformation of C6 at; Warmbloods 30%, Quarter Horses 16% and Thoroughbred horses over 40%.
Aside from the Arabian who is an ancestor to the Thoroughbred, the Warmblood breeds and Quarter Horses all have Thoroughbred lineage in the back line of their breeding. Thus, implying that this condition is heritable as noted by May-Davis [b] and more systemic than just one breed. With this in mind, all critical events should be assessed with the knowledge that a potential congenital malformation could exist in C6, C7 and the 1st sternal rib, as previously noted. With the largest population of horses in Japan being Thoroughbreds, it would be a recommendation to note the studies of several countries including Japan and the severity in percentage of this systemic congenital malformation. Especially in relation to Thoroughbred’ racehorses racing and cornering at speed.
Conclusion
This study showed that of the 4 horses investigated, 3:4 horses displayed a CM of C6, 2:3 displayed the congenital malformation in C6 and C7, and 1:2 a congenital malformation of the 1st sternal rib. Even with a small sample of Thoroughbreds, studies from other countries must be measured and it would therefore be a recommendation to radiograph for this condition in the caudal cervical vertebrae in a pre-purchase examination. The purpose of which would be to eliminate this condition so that riders and handlers are not put at risk.
Author contributions
Sharon May-Davis, Fumiko Minowa and Sadae Monoe wrote and reviewed this article.
Conflict of Interest
The authors have no conflict of interest in the preparation or presentation of this original research article.
Acknowledgement
The author wishes to thank Christine Gee for her professional advice on the manuscript. The Nippon Veterinary and Life Sciences University for the use of their facilities and to those authors / editors/ publishers of those articles, journals and books cited in this manuscript.
References
Derouen A, Spriet M, Aleman M. Prevalance of anatomical of the sixth cervical vertebra and association with vertebral canal stenosis and articular process osteoarthritis in the horse. Vet Radiol Ultrasound, Vol. 00, 2016, pp 1–5.
May-Davis SER. The Occurrence of a Congenital Malformation in the Sixth and Seventh Cervical Vertebrae Predominantly Observed in Thoroughbred Horses. J Equine Vet Sc 2014; 34:1313-17.
May-Davis SER. The Congenital Malformation of the 1st Sternal Rib. J Equine Vet Sc 2014; 34:1313-17.
May-Davis SER, Walker C. Variations and implications of the gross morphology in the Longus colli muscle in Thoroughbred and Thoroughbred derivative horses presenting with a congenital malformation of the sixth and seventh cervical vertebrae. J Equine Vet Sc 2015; 35:560-8.
Santinelli I, Beccati F, Pepe M. Anatomical variation of the spinous and transverse processes in the caudal cervical vertebrae and the first thoracic vertebra in horses. EVJ 48 (2016) 45–49.
Veraa S, Bergmann W, van den Belt A-J, Wijnberg I, Back W. Ex vivo computed tomographic evaluation of morphology variations in equine cervical vertebrae. Vet Radiol Ultrasound, Vol. 00, 1–7.